The medical tech sales model is breaking under the weight of 2026 clinical realities. Physician burnout, private equity clinic consolidation, and the permanent closure of the "drop off donuts at the front desk" access loophole have made the traditional sales development playbook obsolete.
Consider the daily reality of a Sales Development Rep (SDR) at a high-growth medical device or healthcare SaaS company in 2026. Their quota requires them to book twelve product demos per month with orthopedic surgeons, dermatologists, or clinic directors. They are working a list of three hundred target accounts.
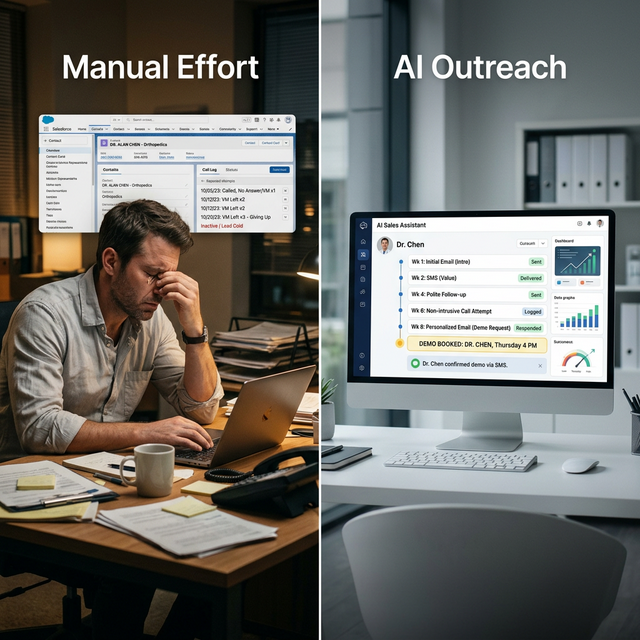
On Monday at 10 AM, the SDR calls Dr. Chen's clinic. A gatekeeper answers, says the doctor is with patients, and sends the call to a general voicemail box. The SDR leaves a message. On Thursday at 2 PM, the SDR tries again. Voicemail. The following Tuesday, the SDR sends an email and follows up with one final call. Voicemail. The SDR logs the activity in the CRM, updates the lead status to "Unresponsive," and moves to the next account.
What the SDR experiences is rejection. What actually happened is that Dr. Chen, who has been managing a post-pandemic patient load that leaves him fourteen minutes to eat lunch at his desk, never even knew the SDR called. The gatekeeper deleted the voicemails because protecting the doctor's time is their primary job metric. The email was buried under seventy-five patient portal notifications.
This is the Ego Depletion boundary in B2B healthcare sales.Human beings are psychologically wired to interpret silence as rejection. After three unreturned touches, a human rep feels like a nuisance. They feel intrusive. Their outreach enthusiasm plummets, their call volume drops, and the medtech company's management responds by buying more lists or writing more aggressive email scripts. Both are the wrong solution to the right problem.
The Mechanics of Polite Persistence
The doctor did not say no. The doctor said nothing. In medical sales, a non-response is a scheduling conflict, not a product rejection. The only way to penetrate a calendar that is booked in fifteen-minute increments months in advance is asynchronous, high-stamina persistence.
An AI outreach agent does not experience ego depletion. It does not feel awkward leaving a fourth message. It does not get demoralized when an email goes unread. It simply executes the math of statistical probability.
The concept ofPolite Persistencerelies on treating the outreach sequence not as a sprint to a "no," but as a marathon to a "this is finally a convenient moment." If a human SDR gives up at touch number three, they have surrendered the account right before the probability curve actually begins to work in their favor. An AI agent is programmed to make touch number four in week three. Touch number five in week five. Touch number six in week eight.
And because the AI is not fatigued, every touch remains perfectly polite, deferential, and context-aware. "Hi Dr. Chen, I know clinic volume is exceptionally high right now. Just rising to the top of your inbox regarding the new imaging integration - no reply needed until you have a breathing moment." This approach stops being an interruption and starts becoming a reliable, patient presence. Eventually, Dr. Chen completes a Friday afternoon surgery early, checks his messages, and replies: "Send me a link for next Thursday morning."
Getting Through the Healthcare Access Layer
Persistence alone is insufficient if the channel strategy is wrong. Calling a clinic's main line is the lowest-probability outreach method in modern medtech sales, yet it remains the default behavior for thousands of SDRs.
A clinic's phone system is explicitly designed to keep salespeople away from the physician. That is its architectural purpose. The phone tree routes to a receptionist whose primary directive is patient care, and whose secondary directive is deflecting unsolicited vendors. To reach the medical decision-maker, the outreach must happen on the channels the physician actually monitors between patients.
The difference between a medical practitioner and a corporate executive is that the physician is entirely governed by the clinical schedule. They are not sitting at a desk checking a centralized inbox throughout the day. They have brief, fragmented windows of digital availability - three minutes between a complex consultation and a routine follow-up, ten minutes while eating a sandwich at their desk, and perhaps forty-five minutes on Sunday evening. The omnichannel strategy must map precisely to these fragmentation windows.
Email timing:An AI agent analyzing open rates across the healthcare sector knows that the highest probability of a physician reading an email is between 6:15 AM and 7:00 AM (before morning rounds) or Sunday evening between 7:00 PM and 9:00 PM (when prepping for the week). A human SDR works 9 to 5. If the human rep sends an email at 10 AM on a Tuesday, by the time the doctor checks their inbox at 6 PM, that email has been buried beneath eighty patient portal notifications, internal clinic memos, and lab results. The AI agent schedules the email perfectly for Sunday at 7:14 PM, ensuring it is the first undigested item the doctor sees.
Professional SMS:While cold texting a physician's personal cell phone is a high-risk compliance and relationship violation, professional SMS to a direct clinic line or business-provided mobile device is increasingly effective if the tone is strictly deferential. The AI can manage SMS threads where a doctor might reply with a single "Yes, interested, talk to Sarah upfront." The AI immediately pivots, contacts Sarah, references the doctor's explicit instruction, and books the demo.
LinkedIn connection sequencing:The AI can coordinate connection requests and value-add content sharing on professional networks, creating a surround-sound effect where the doctor sees the brand name multiple times before the crucial email arrives. For medical device sales, this often involves sharing peer-reviewed studies or clinical outcome data. The physician sees the study attached to the AI's profile on LinkedIn, subconsciously registers the company name, and is therefore primed to open the email that arrives three days later.
The synthesis of these channels creates a persistent but non-invasive presence. The doctor never feels harassed by aggressive cold calling, yet the medtech product remains consistently surfaced at the exact moments the doctor is capable of engaging.
The Economics of Consistent SDR Follow-Up
The mathematical argument for AI outreach in medtech sales is devastating to the traditional heavy-headcount SDR model. The math does not merely suggest a marginal efficiency gain; it reveals a structural flaw in how most medical technology companies build their go-to-market teams.
A medical device or healthcare SaaS company selling a $40,000 capital equipment package might employ five SDRs at a fully loaded cost of $85,000 each per year ($425,000 total). Those five reps might generate eighty booked demos a month combined. Their capacity is capped by the number of dials they can make, the time spent leaving voicemails, the administrative burden of logging activities in Salesforce, and the psychological weight of constant rejection.
That psychological weight is not a soft metric. It is the primary driver of SDR turnover, which in the medical sales sector averages just fourteen months. Every time a rep leaves, the medtech company loses three months to recruiting, three months to onboarding, and thousands of dollars in lost pipeline momentum. The cost of human outreach is staggering when fully accounted for.
An AI outreach deployment can work a list of 10,000 target clinics simultaneously. It can personalize every single touchpoint based on the clinic's specialty, size, location, and even the specific medical procedures they advertise. It handles the early morning emails, the Sunday night follow-ups, and the week-eight polite nudges automatically. It filters the "unsubscribe" and "not interested" replies instantly, without emotion.
The human sales team is not replaced;they are elevated.Instead of making three hundred cold calls to book two meetings, the human Account Executives (AEs) spend 100 percent of their time conducting actual product demonstrations with doctors who have already agreed to the meeting. The AI handles the grueling top-of-funnel friction; the human handles the high-empathy, complex clinical presentation that closes a $40,000 deal.
By removing the capacity constraints of the SDR layer, the medtech company can scale its top-of-funnel outreach infinitely without adding a single dollar to its payroll. A new product launch no longer requires hiring and training a new cohort of SDRs. The company simply reconfigures the AI outreach parameters and launches the campaign to forty thousand medical practitioners overnight. The AEs arrive on Monday morning to a calendar booked with highly qualified demonstrations.
FAQ
Do doctors respond negatively to automated outreach if they realize it is AI?
Physicians are highly analytical and extremely protective of their time. They generally resent bad outreach - human or automated - that wastes their time with generic pitches or aggressive presumptive closes. They rarely resent polite, concise, relevant outreach that clearly states the clinical or financial value proposition and allows them to respond on their own schedule. Transparency is important; the AI should introduce itself as a digital assistant for the medtech firm. When a doctor realizes a system has politely followed up six times without being annoying, they often recognize the operational efficiency of the medtech company itself. The physician respects the persistence, provided it is respectful of their clinical schedule.
How does AI-supported follow-up handle gatekeepers and clinic administrators?
In many B2B healthcare sales scenarios, the practice manager or clinical director is actually the superior initial target compared to the physician. The AI outreach sequences are often multi-threaded. The AI emails the physician with a clinical value proposition ("improving patient outcomes in peripheral neuropathy") while simultaneously emailing the practice manager with the operational value proposition ("reducing imaging wait times by 14% and standardizing medical billing workflows"). When one replies, the AI coordinates the calendar invite for both stakeholders, ensuring the entire decision-making unit is present for the human AE's demo. This multi-threaded capability is almost impossible for an overworked human SDR to sustain at scale.
The Lobby Fatigue Problem: Why Traditional SDR Models Stall
Ask any MedTech sales founder about their biggest "untracked" expense, and they won't point to their CRM or their travel budget. They'll talk about "Lobby Fatigue."
Imagine your top-performing sales rep, Mike. Mike has spent weeks trying to get a 10-minute demo for a new robotic surgical tool with Dr. Thompson, a high-volume orthopedic surgeon. He finally scores a "tentative" 10:00 AM coffee meeting at the hospital's cafe.
Mike shows up at 9:45 AM. At 10:15 AM, the surgical assistant calls: "Sorry, Mike. Dr. Thompson hit a complication in the first procedure. He's back in the OR for at least two more hours. We'll have to reschedule."
Mike leaves. He just wasted three hours of travel and preparation time. But the real cost isn't the three hours; it's the "Emotional Debt." Mike is now less likely to chase Dr. Thompson aggressively for the reschedule because he associates that account with friction and failure.
This is where the humanized SDR model breaks down.Humans have a limited capacity for rejection and "operational ghosting." Every time a surgeon cancels, a little bit of your sales rep's momentum dies.
The Assistant-as-an-Ally Strategy
We often talk about "Gatekeepers" as the enemy. But in medical sales, the Medical Assistant (MA) or the Office Manager is the most overworked person in the building. They aren't trying to block you; they are trying to protect their surgeon's sanity.
A relatable AI intake or outreach system doesn't try to "bypass" the assistant. It tries to **solve their scheduling headache.** By offering a frictionless, 24/7 self-service portal where the assistant can instantly find a 15-minute window that works for the surgeon-without a five-email chain-you aren't a "sales tool." You are a utility.
When the MD finally walks into that demo, they aren't irritated by the "sales follow-up." They are impressed that your company respects their time so much that you've automated the friction away. That is the "Quiet Protocol" in action-it makes the owner look sophisticated, not desperate.
Is this compliant with healthcare marketing regulations?
Yes, standard B2B outreach compliance (CAN-SPAM, etc.) applies. Since the medtech company is conducting business-to-business sales targeting clinical entities, and is not marketing medical services to consumers or sharing Protected Health Information (PHI), standard commercial outreach rules govern. The AI is simply automating the exact same email and scheduling workflows that a human SDR would be executing, but doing so with perfect consistency and scheduling precision. A well-configured AI actually reduces compliance risk compared to a rogue human SDR, because the AI never strays from approved messaging matrices and rigorously honors standard opt-out classifications.
What is the typical time-to-value for an AI-supported SDR deployment in medical sales?
MedTech companies typically see the first wave of booked demos within fourteen to twenty-one days of deployment. The immediate lift comes from engaging the low-hanging fruit - physicians who were already problem-aware but had simply ignored previous human outreach because the timing was inconvenient. However, the true ROI compounding effect occurs between days sixty and ninety. This is when the Polite Persistence engine reaches the fifth and sixth touchpoints on accounts that human SDRs would have abandoned a month ago. The bookings generated in month three are composed almost entirely of leads that would have been marked "cold" in a traditional human-only sales model.
Use your own records before you decide
Source: start with your call log, CRM notes, booking calendar, missed-call records, web form timestamps, and Google Business Profile. Those records show whether buyers reached you, how fast they heard back, what they asked for, and where the next step broke down.
For seven days, mark each missed call, late reply, unbooked form, stale estimate, and review request that never went out. That small sample gives an owner a practical picture of the front-door gap before they spend more on ads, software, or staff.
The loss estimate is basic business math, not a magic claim.
Revenue-leak examples on this site are built from visible operating inputs: inquiry volume, missed-call or slow-response rate, booking rate, average job or client value, repeat value, and follow-up recovery. The fastest way to make the number real is to run the diagnostic for your closest business type, then compare it against your own call log, CRM, booking calendar, form timestamps, and review activity.
Use this before you buy another tool.
Pull one recent week of calls, forms, chats, and booking requests. Mark every inquiry that waited, went unanswered, needed a manual reminder, or never reached a clear next step. That simple review shows whether the problem is demand, staffing, or the front-door system.
If those answers are hard to find, that is the first issue to fix. The Quiet Protocol installs the system that answers faster, routes cleaner, books more of the right demand, requests reviews, and keeps follow-up from depending on memory.

Vikram Roy is the founder of The Quiet Protocol, a Toronto-based AI systems firm serving service businesses across the Greater Toronto Area, Canada, and the United States. He works directly with home service companies, dental practices, clinics, and local businesses to install AI operating systems that capture more leads, reduce no-shows, grow reviews, and recover revenue without adding manual overhead. All content is written from Toronto, Ontario. Connect on LinkedIn →
See the system page tied most closely to the problem this article is diagnosing.
Specialty ClinicsOpen the industry path where this revenue leak is framed in operational terms.
Run Revenue Leak DiagnosticQuantify the leak before you decide what type of system needs to be installed.
Call the AI Receptionist DemoHear the receptionist live, give it your business context, and test a short caller roleplay before you book.
Results & ProofReview what the system changes once the front door is rebuilt around response and continuity.

Real Estate Brokerages: The AI ISA That Follows Up With Zillow Leads After Hours
The research on real estate lead response is unambiguous and has been replicated across hundreds of studies. A prospect who submits an online inquiry and is contacted within five minutes is eight times more likely to convert than one contacted thirty minutes later. A prospect contacted on Monday morning for a Sunday night submission is, for the majority of brokerages, already lost. The math of online lead conversion in real estate is not complicated - it is just brutally unforgiving, and it operates equally aggressively at 10 PM on a Sunday as it does at 2 PM on a Tuesday. Most real estate brokerages are built for 2 PM on a Tuesday.
Stop Buying Local Service Leads: Fix Your Intake Infrastructure Before You Buy Another Ad
Bad lead quality is not always the problem. Many service businesses lose paid leads because callbacks are slow, after-hours intake is weak, and follow-up is inconsistent.

Plastic Surgery Clinics: Discretion and Speed in High-Ticket Intake
Cosmetic procedure demand in 2025 and 2026 has reached historic highs. Post-pandemic, the category of elective aesthetic investment has normalized across income brackets that were previously not in the market. The demand exists. The prospects are searching. What the research on high-ticket cosmetic intake consistently shows is that the loss is almost never happening at the surgeon quality level - it is happening at the first contact point, in the first ninety seconds of an inquiry, when a called-on-hold prospect or a cold clinical voice produces the friction that sends a $12,000 rhinoplasty inquiry to a competitor. The plastic surgery clinic that has solved intake has solved the most solvable problem in its revenue stack.
Calculate the revenue leak.
Stop guessing. See how much demand your business may be losing through missed calls, slow replies, weak booking, review gaps, and follow-up drag, then decide whether Voice AI is the right system path.
Run the calculationPrefer to hear it first?
Call the live AI receptionist and test the conversation.
Call the live AI receptionist anytime. Tell it about specialty clinics, then hear a short live roleplay based on the calls your front desk actually gets.